Psoas and Iliacus: The Complete Anatomy Guide (And Why These Two Muscles Matter)
The psoas and iliacus are two separate muscles that form the iliopsoas complex — the primary hip flexor and a key stabilizer of the lumbar spine. The psoas originates from the lumbar vertebrae (T12–L5); the iliacus originates from inside the hip bone. Because they attach to different structures, they can develop tightness independently and each responds best to its own targeted release work.
In This Article
 The psoas sits deep in the abdomen, right against the front of the lumbar spine. Most people don’t know it’s there.
The psoas sits deep in the abdomen, right against the front of the lumbar spine. Most people don’t know it’s there.
If you’ve landed here, you’re probably trying to figure out what the “psoas” is — or maybe a physical therapist mentioned something about the “iliacus” or “iliopsoas.” These are the two muscles that keep coming up when people search for answers to recurring lower-back and hip tightness.
This guide covers both muscles — where they are, what they do, what sitting changes, and why addressing both of them (not just one) matters. All in language that doesn’t require a medical degree to understand.
Where Is the Psoas?
The psoas major (pronounced “SO-az”) is a long, thick muscle that runs from the front of the lower spine to the top of the thigh bone.
- Origin: The vertebral bodies and transverse processes of T12 through L5 — the bottom of the thoracic spine through all five lumbar vertebrae
- Insertion: The lesser trochanter of the femur — a bony bump on the inside of the upper thigh bone
Think of it as a rope connecting the lower back to the leg, running through the center of the body. It’s the only muscle that directly bridges the upper and lower body.
You can’t feel it from your back — it sits deep, right against the front of the spine, behind the abdominal organs. It can be accessed from the front by pressing gently inward beside the navel, but most people don’t know it’s there.
CDN shared asset — anatomy-psoas-iliacus.png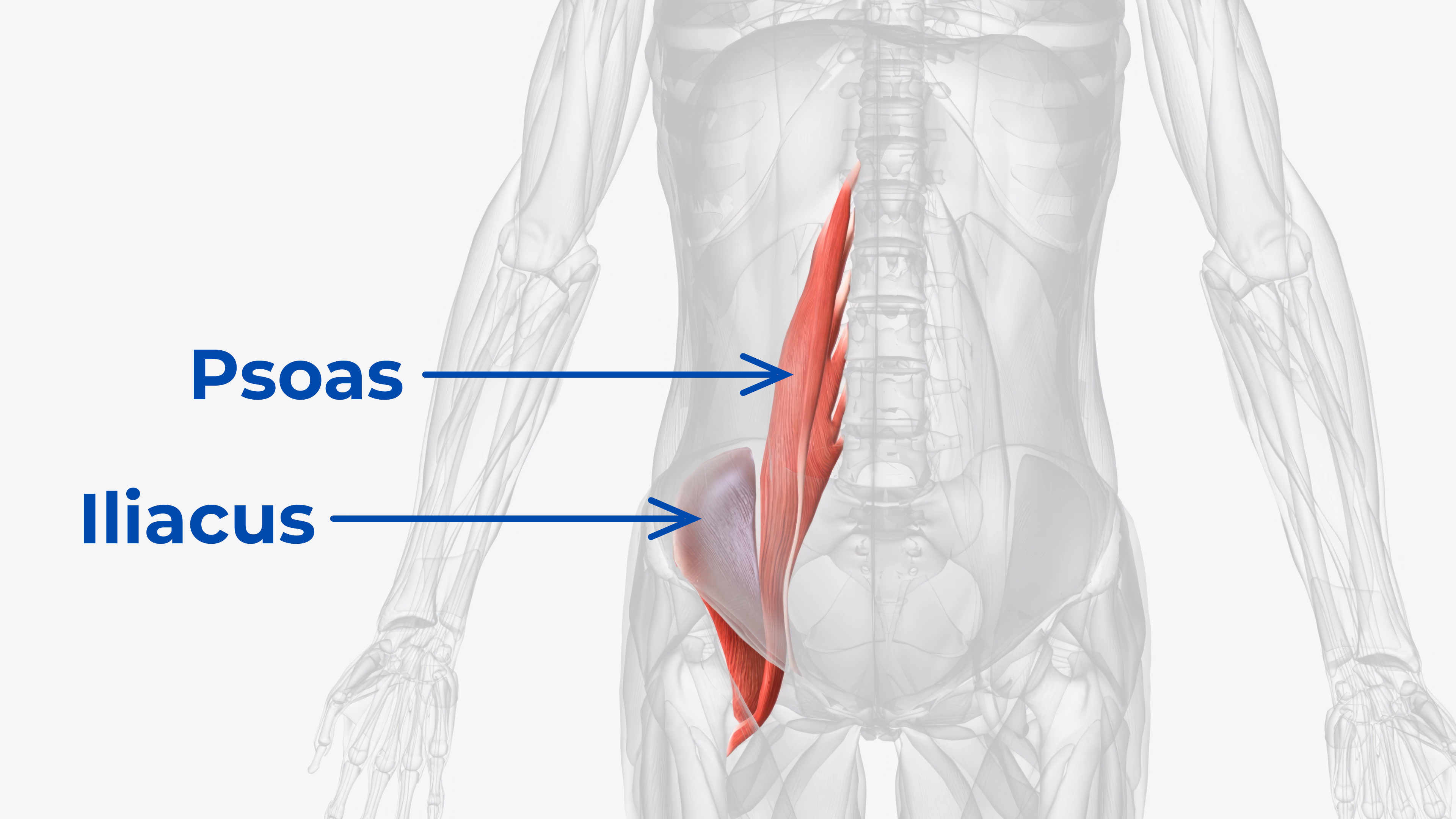 The psoas originates from T12–L5; the iliacus originates from the iliac fossa. Both insert at the lesser trochanter of the femur.
The psoas originates from T12–L5; the iliacus originates from the iliac fossa. Both insert at the lesser trochanter of the femur.
The Iliopsoas Complex: Two Muscles, One Function
The psoas major rarely works alone. It has a partner: the iliacus. The iliacus originates from the iliac fossa — the inner, bowl-shaped surface of the hip bone. It joins the psoas tendon and inserts at the same point on the femur.
Together, they form the iliopsoas complex:
| Feature | Psoas Major | Iliacus |
|---|---|---|
| Origin | Lumbar spine (T12–L5) | Iliac fossa (inside hip bone) |
| Insertion | Lesser trochanter (femur) | Lesser trochanter (femur) |
| Primary Pull | Spine → leg (spinal stability + hip flexion) | Pelvis → leg (pelvic stability + hip flexion) |
| Access Point | Abdomen, beside the navel | Inside the hip bone (iliac fossa) |
| Release Tip Needed | Broad, firm, sustained pressure | Narrow, angled pressure into the hip bone |
Because they originate from different structures, they can be tight independently. A locked psoas with a relatively mobile iliacus, or vice versa, is common. This is why approaches that work on them as a single unit — like standard hip-flexor stretches — often miss part of the pattern.
What the Psoas Does: Four Critical Functions
1. Hip Flexion (Primary)
The psoas is the strongest hip flexor in the body. Every time a knee lifts — walking, running, climbing stairs, getting out of a chair — the psoas initiates the movement. Without it, the thigh couldn’t be brought toward the torso.
2. Lumbar Spine Stabilization
Because it attaches to every lumbar vertebra, the psoas acts as a deep anterior stabilizer of the spine. It helps maintain the natural lumbar curve (lordosis) and keeps the vertebrae aligned during movement.
When it functions properly, this stabilization is invisible. When it’s persistently shortened from long sitting, it can pull the spine into an exaggerated arch and add load to the lower back.
3. Spinal Rotation and Lateral Flexion
The psoas assists in rotating the trunk (twisting) and bending to the side. It works in concert with the quadratus lumborum, multifidus, and obliques to produce controlled spinal movement.
4. Postural Maintenance
The psoas is tonically active during upright standing. It’s one of the muscles keeping the body from collapsing forward, working below conscious awareness as part of the deep postural system.
Bonus function — breathing: The psoas shares fascial connections with the diaphragm at T12. Ongoing psoas tension can restrict diaphragmatic movement, contributing to shallow breathing patterns. Many people report deeper breathing after psoas release.
AI-generated (Nano Banana Pro) — Black Core Nexus on PT approach table with foam roller and resistance bands, clinical setting → uploaded as article-pp06-product.webp The Core Nexus features two anatomically distinct tips — one for the psoas, one for the iliacus — used in clinical and home settings alike.
The Core Nexus features two anatomically distinct tips — one for the psoas, one for the iliacus — used in clinical and home settings alike.
The Iliacus: The Forgotten Half
Most discussions about the psoas ignore the iliacus entirely — or lump both together as “the hip flexors.” But the iliacus matters independently:
The psoas attaches to the spine. The iliacus attaches to the pelvis.
This means they can be tight independently of each other. And because they attach to different structures, each responds best to its own targeted release work.
- The psoas responds to broader pressure through the abdomen
- The iliacus requires a narrow, angled approach inside the hip bone
- One stretch can’t provide both types of pressure
This is one of the key reasons standard hip-flexor stretches don’t fully address the pattern. They lengthen both muscles together but can’t apply the specific, targeted pressure each needs individually.
What Sitting Changes
The psoas is in its shortened position when the hip is flexed — like when sitting. For many people, that’s six to eight hours a day or more.
Over time, both muscles adapt to this shortened position:
- Muscle fibers remodel to accommodate the new length
- Fascia surrounding the muscles becomes dehydrated and restrictive
- tight spots develop within the muscle belly
The result is a psoas and iliacus that stay shortened even when standing. The psoas pulls the lumbar spine forward into an exaggerated arch. The iliacus tilts the pelvis forward. Together, this dual pull adds load and tension that most back-focused routines miss — because they only work on one of the two muscles, or neither.
===== SECTION: HOW TO address IT =====How to Work on It
The approaches that help most, in order of usefulness:
1. Direct myofascial release — sustained, targeted pressure applied directly to the psoas and iliacus independently. This works on tight spots, supports fascial mobility, and helps each muscle reset its resting length. Requires a tool designed for the depth and angle needed (foam rollers can’t reach the psoas).
2. Contract-relax (PNF) stretching — active engagement followed by passive stretch. More effective than static stretching alone because it leverages the nervous system’s the brake effect reflex.
3. Movement restoration — walking, standing desks, frequent position changes. Addresses the position pattern (prolonged hip flexion) rather than just the surface sensation.
What doesn’t work well:
- Static hip flexor stretches alone (kneeling lunges, pigeon pose)
- Foam rolling (too broad, too shallow to reach either muscle)
- Core strengthening alone (important for maintenance but doesn’t release the psoas)
- Ignoring it (adaptive shortening is progressive)
The most effective approach starts with self-myofascial release using a tool with muscle-specific tips for both the psoas and iliacus. The Core Nexus was designed for exactly this — two anatomically distinct tips, each shaped for its target muscle, with a self-rotating base for hands-free angle adjustment. The buyer’s guide explains what to look for in detail.
Ready to release both muscles?
The Bottom Line
The psoas and iliacus are two of the most anatomically significant muscles in the body — and two of the most misunderstood. The psoas runs from the lumbar spine to the femur, controlling hip flexion and spinal stability. The iliacus lines the inside of the hip bone and controls pelvic stability. Together, they form the iliopsoas complex.
Because they originate from different structures, they develop tightness independently and each responds best to its own release work. The psoas needs broad, deep abdominal pressure. The iliacus needs narrow, angled pressure directed into the hip bone. One-size-fits-all approaches — stretching, foam rolling, generic tools — can’t provide both.
Understanding this anatomy is the first step toward easing the recurring hip-flexor and lower-back tightness that conventional stretching alone tends to miss.
Endorsed by Clinicians
 Dr. Goñi
MD — Sports Medicine
Dr. Goñi
MD — Sports Medicine
 Dr. Sosa
DC — Chiropractic
Dr. Sosa
DC — Chiropractic
 Dr. Lang
PT, DPT — Physical Therapy
Dr. Lang
PT, DPT — Physical Therapy
 Dr. McHale
DC — Chiropractic
Dr. McHale
DC — Chiropractic
 Dr. Steph Dorworth
PT, DPT — Physical Therapy
Dr. Steph Dorworth
PT, DPT — Physical Therapy
Frequently Asked Questions
The iliopsoas is the combined name for the psoas major and iliacus muscles. They merge into a common tendon that attaches to the femur. While they function as a team for hip flexion, they originate from different structures (spine vs. hip bone) and can develop tightness independently.
Yes. The psoas and diaphragm share fascial connections at the T12 vertebra. Ongoing psoas tension can restrict diaphragmatic movement, contributing to shallow, chest-dominant breathing. Many people report deeper breathing after sustained psoas release.
No. The psoas minor is present in roughly 40–60% of the population. It’s a much smaller muscle running from T12/L1 to the pubic bone and plays a minor role in spinal flexion. Its absence is not clinically significant.
The psoas sits deep in the abdomen, right against the front of the lumbar spine. A foam roller is designed for superficial muscles on the outside of the body. It cannot penetrate deeply enough through the abdominal wall to apply meaningful pressure to the psoas. The iliacus is even harder to reach — it sits inside the bowl of the hip bone.
If tightness centers in the lower back with an exaggerated arch, the psoas is more likely involved (it pulls the spine forward). If the pelvis sits tilted forward with hip-dominant tightness, the iliacus may be the bigger contributor. In most cases of recurring tightness, both are involved — so working on both is the simplest approach.
Psoas release involves broad, firm pressure applied through the abdomen, beside the navel. Iliacus release requires a narrow, angled tip directed into the iliac fossa (inside the hip bone). The two techniques target different structures at different angles — which is why a tool needs distinct tip shapes for each.
Nexus Health Tools designs precision instruments for targeted myofascial release, built on real anatomy and endorsed by clinicians. Every product is engineered in the USA to address the muscles most tools miss.