Why Foam Rolling Won't Fix Tight Hip Flexors (And What Actually Works)
Foam rollers are effective for superficial muscles like quads and hamstrings, but they physically cannot reach the psoas or iliacus — the two deep hip flexor muscles responsible for most chronic hip tightness. These muscles sit behind the abdominal organs (psoas) and inside the hip bone (iliacus), beyond the reach of broad, surface-level pressure. Targeted release with anatomically shaped tools is what actually works.
In This Article
 Foam rollers work for quads and hamstrings. But the muscles causing most hip flexor tightness sit too deep to reach this way.
Foam rollers work for quads and hamstrings. But the muscles causing most hip flexor tightness sit too deep to reach this way.
Foam Rolling Works — Just Not Here
Foam rollers are one of the most effective self-care tools for superficial muscles. Quads, hamstrings, IT band, calves, upper back — all respond well to the broad, rolling pressure a foam roller provides.
But the hip flexors are a different story.
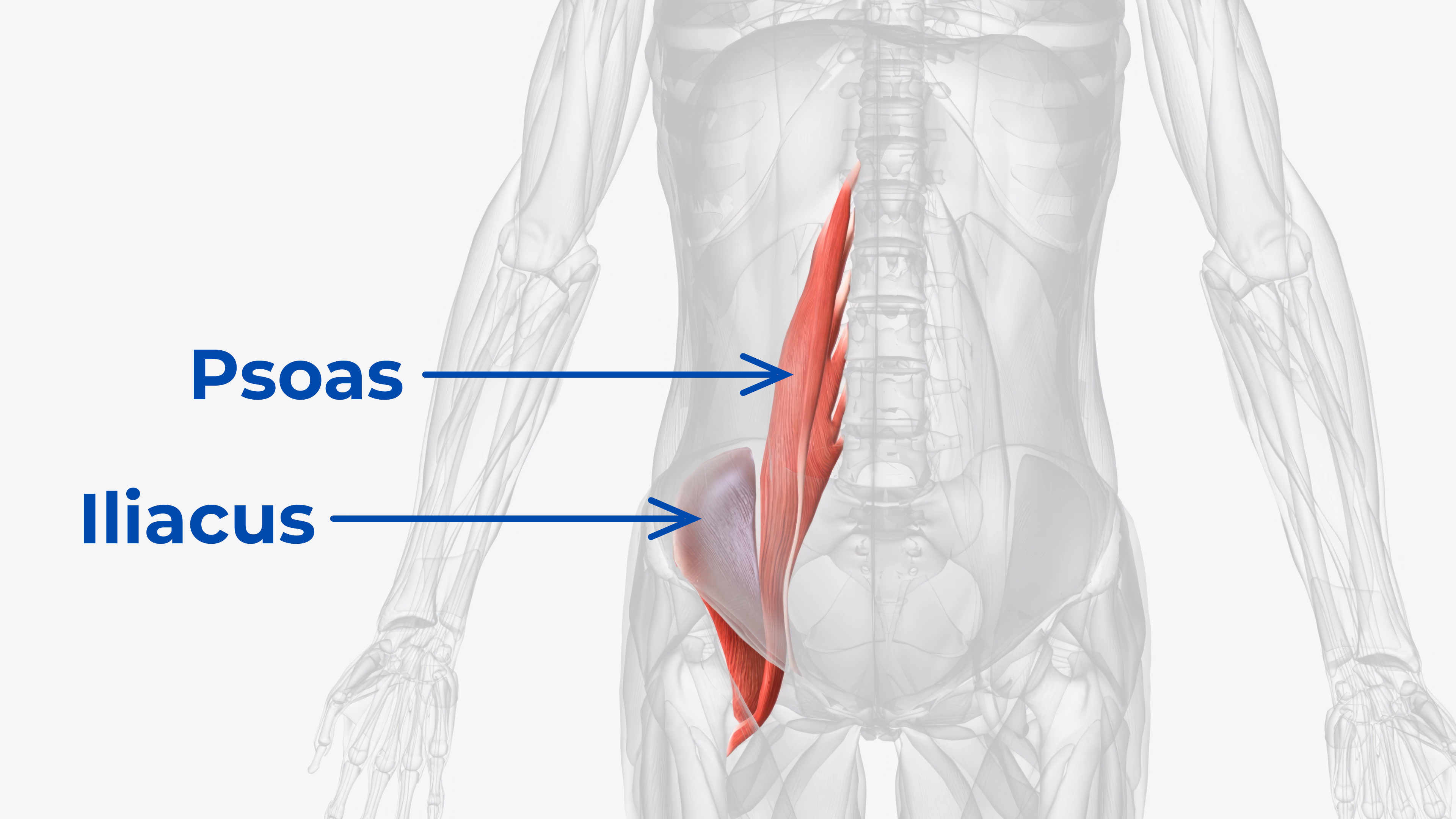
The primary hip flexors — the psoas and the iliacus — sit deep inside the body. The psoas runs along the front of the lumbar spine, buried beneath the abdominal organs. The iliacus lines the inside of the hip bone. Neither muscle is accessible from the body’s surface where a foam roller makes contact.
This isn’t a technique issue. It’s a physics issue.
The Physics Problem
A foam roller applies pressure by compressing tissue between the roller and the floor. This works when the target muscle is between the body surface and a hard surface — like rolling the quad against the ground.
The psoas is not between the surface and the ground. It’s behind the intestines, along the spine. A foam roller pressing on the abdomen would need to compress through multiple layers of abdominal muscle, fascia, and organs to reach it — which doesn’t happen. The pressure dissipates across the broad surface of the roller long before it reaches the psoas.
The iliacus is even more inaccessible. It sits inside the bowl of the hip bone — the iliac fossa. There is no angle from which a foam roller can reach inside this concave surface. The hip bone itself blocks the path.
 The psoas runs along the lumbar spine behind the organs. The iliacus lines the inside of the hip bone. Neither is reachable from the body’s surface.
The psoas runs along the lumbar spine behind the organs. The iliacus lines the inside of the hip bone. Neither is reachable from the body’s surface.
What About Lacrosse Balls?
Lacrosse balls and similar hard balls are better than foam rollers for deep work because they concentrate pressure into a smaller area. Some people use them for psoas release by lying face-down and positioning the ball near the hip crease.
This can partially work for the psoas — the smaller contact area allows deeper penetration. But there are significant limitations:
- No stability: The ball rolls away from the target area, requiring constant repositioning
- Imprecise: The round shape doesn’t conform to the psoas anatomy — it applies pressure in a circle when the muscle runs in a line
- Iliacus: still unreachable. A round ball cannot navigate inside the curved surface of the hip bone. The geometry simply doesn’t work.
- No rotation: Static pressure from a ball misses the benefit of releasing while the muscle is engaged through leg movement
Lacrosse balls are a step up from foam rollers for the psoas. But they still can’t reach the iliacus, and they sacrifice stability and precision for their simplicity.
What Actually Works
Effective hip flexor release requires four things that foam rollers and lacrosse balls cannot provide:
- Targeted, sustained pressure — not rolling, but static or slow-moving compression directly on the muscle belly
- Different shapes for different muscles — the psoas needs broader contact; the iliacus needs a narrow, angled approach that can reach inside the hip bone
- Stability — the tool needs to stay in place while body weight settles onto it
- Movement-based release — engaging the muscle through leg rotation while under pressure produces deeper release than static pressure alone
 The difference between broad surface pressure (foam roller) and targeted anatomical precision (Core Nexus). Different tools for different muscles.
The difference between broad surface pressure (foam roller) and targeted anatomical precision (Core Nexus). Different tools for different muscles.
This is why purpose-built psoas and iliacus release tools exist. Unlike foam rollers, they’re designed with separate tips shaped for each muscle’s specific anatomy — because the psoas and iliacus are in different locations and need different pressure approaches. The Core Nexus uses muscle-specific tips (one shaped for the psoas, one contoured for the iliacus) and a self-rotating base for movement-based release. A tool that only addresses one muscle leaves half the problem untreated.
The Role of Stretching
Stretching complements tool-based release but doesn’t replace it. A classic hip flexor stretch (like a kneeling lunge) lengthens the iliopsoas at the muscle-tendon junction. This provides temporary relief and improved range of motion.
However, stretching doesn’t address trigger points — localized knots of contracted muscle fiber within the muscle belly. These trigger points are what cause the chronic, recurring tightness that stretching temporarily alleviates but never fully resolves.
How Release Methods Compare
| Method | Reaches Psoas | Reaches Iliacus | Stable | Allows Movement |
|---|---|---|---|---|
| Foam Roller | ✘︎ | ✘︎ | ✔︎ | ~ |
| Lacrosse Ball | ~ | ✘︎ | ✘︎ | ✘︎ |
| Hip Flexor Stretching | ~ | ~ | N/A | N/A |
| Massage Therapy | ✔︎ | ~ | ✔︎ | ✘︎ |
| Psoas-Only Tool | ✔︎ | ✘︎ | ✔︎ | ~ |
| Core Nexus | ✔︎ | ✔︎ | ✔︎ | ✔︎ |
A Better Approach
For lasting hip flexor relief, the protocol is straightforward:
- Release the psoas with broad, sustained pressure — hold until the tissue begins to soften and yield
- Release the iliacus with narrow, angled pressure inside the hip bone — same approach, hold until the tissue responds
- Stretch the hip flexors after releasing — the stretch will be significantly more effective once the trigger points have been addressed
- Repeat daily for several weeks to create lasting change in chronic tension patterns
Both muscles must be addressed. Releasing the psoas without the iliacus (or vice versa) leaves half the system tight, and the released muscle will tighten back up because the other is still pulling the pelvis out of alignment.
The Bottom Line
Foam rollers are excellent tools — for the right muscles. But they physically cannot reach the psoas or the iliacus, the two muscles most responsible for chronic hip flexor tightness and the lower back pain, anterior pelvic tilt, and reduced mobility that follow.
Lacrosse balls get closer but still can’t reach the iliacus and lack the stability for effective sustained release. Stretching helps but doesn’t address trigger points.
The most complete approach combines targeted, muscle-specific pressure with stretching — releasing the trigger points first so the muscles can actually lengthen. Both the psoas and the iliacus need to be addressed for lasting results.
Ready to release both muscles?
Endorsed by Clinicians
 Dr. Goñi
MD — Sports Medicine
Dr. Goñi
MD — Sports Medicine
 Dr. Sosa
DC — Chiropractic
Dr. Sosa
DC — Chiropractic
 Dr. Lang
PT, DPT — Physical Therapy
Dr. Lang
PT, DPT — Physical Therapy
 Dr. McHale
DC — Chiropractic
Dr. McHale
DC — Chiropractic
 Dr. Lein
PT, DPT — Physical Therapy
Dr. Lein
PT, DPT — Physical Therapy
Frequently Asked Questions
The psoas runs along the front of the lumbar spine, behind the abdominal organs. A foam roller applies broad, surface-level pressure that dissipates across the abdomen long before it reaches the depth of the psoas. The muscle is simply too deep and too far from the body’s surface for a foam roller to access.
Certain stretches (like the kneeling hip flexor stretch or constructive rest position) can help lengthen the psoas, and some yoga poses can encourage the muscle to relax. However, these methods don’t apply direct pressure to trigger points within the muscle belly. For chronic tightness with trigger points, direct pressure from a tool combined with stretching produces more complete results.
Yes — just not for the hip flexors themselves. Foam rolling the quads, IT band, and hamstrings is valuable for overall hip mobility and can complement targeted psoas and iliacus release. The issue isn’t that foam rollers are bad tools — they’re excellent for the muscles they can reach. They just can’t reach the psoas or iliacus.
The psoas originates on the lumbar spine and passes through the abdominal cavity. The iliacus originates on the inside surface of the hip bone (iliac fossa). They attach to the same point on the femur and work together to flex the hip, but their different locations mean they require different release techniques — the psoas through the abdomen, the iliacus through the inside of the hip bone.
After. Release the trigger points with direct pressure first, then stretch. When the muscle has active trigger points (tight knots), stretching can only lengthen the healthy fibers around the knot — the trigger point itself doesn’t stretch. Releasing first allows the entire muscle to lengthen uniformly when stretched.
Daily release for 2–5 minutes per side is the most effective protocol for chronic tightness. Consistency matters more than duration — brief daily sessions produce better results than occasional long sessions. Most people notice meaningful changes within 2–3 weeks of consistent daily practice.
Nexus Health Tools designs precision instruments for targeted myofascial release, built on real anatomy and endorsed by clinicians. Every product is engineered in the USA to address the muscles most tools miss.
This article is for educational purposes only. If you have persistent pain, consult a qualified healthcare provider.