Pelvic Floor Tension and the Psoas-Iliacus Connection: What Postpartum Recovery Missed
Lingering pelvic tension that persists after Kegels and pelvic floor work often involves the psoas and iliacus — two deep hip flexor muscles that are fascially connected to the pelvic floor. Pregnancy and the postpartum months tighten both muscles, pulling the pelvic floor into an overly tight, guarded state that won’t ease with strengthening alone. Releasing the psoas and iliacus can help when pelvic floor recovery has plateaued.

Core Nexus
Two muscles. Two tips. One tool — releases both the psoas and the iliacus.
In This Article
 Pelvic floor exercises work on one piece. But if the psoas and iliacus are pulling on the pelvic floor from above, an upstream source of tension hasn’t been touched.
Pelvic floor exercises work on one piece. But if the psoas and iliacus are pulling on the pelvic floor from above, an upstream source of tension hasn’t been touched.
The Missing Piece in Pelvic Floor Recovery
The Kegels have been done. Maybe pelvic floor physical therapy too. Breathing exercises, posture corrections, hip bridges. Things are better — but not fully settled.
For many women in the postpartum months, this plateau is where progress stalls. The pelvic floor itself has been thoroughly addressed, but the sensations persist: lingering pelvic tension, a sense of heaviness, discomfort with certain movements, or a pelvic floor that won’t fully relax after contracting.
There’s a reason this happens. And it has nothing to do with doing Kegels wrong or needing more of them.
There are two muscles — the psoas and the iliacus — that are directly connected to the pelvic floor through fascia, nerve pathways, and shared biomechanics. They sit deep in the abdomen and pelvis, adjacent to the pelvic floor muscles. And if they’re persistently tight (which they very often are after pregnancy, delivery, and the sitting-heavy early months of motherhood), they may be pulling on the very structures that pelvic floor work is trying to support.
How the Psoas and Iliacus Connect to the Pelvic Floor
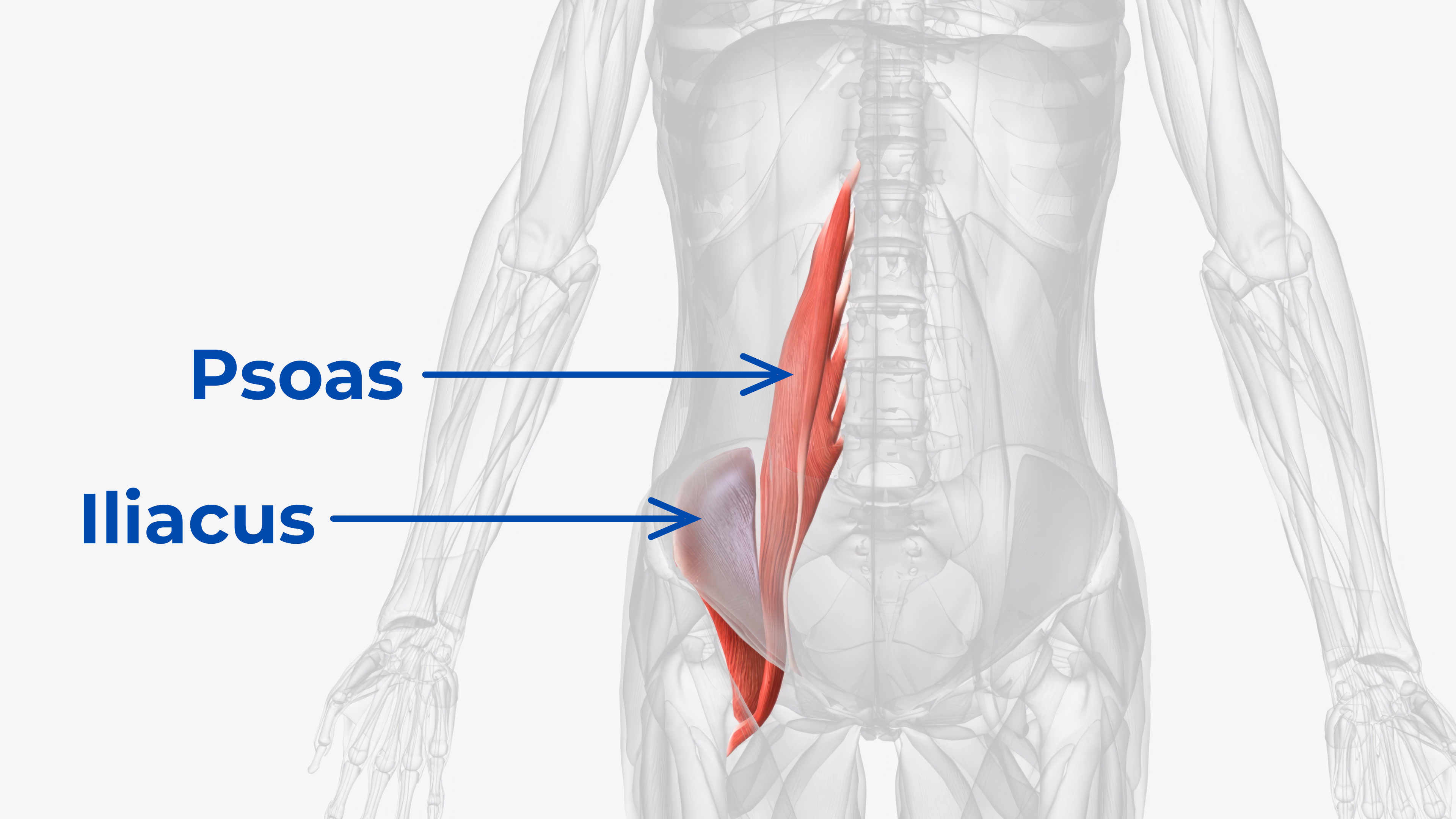
The psoas runs from the front of the lumbar spine (T12–L5) down through the pelvis to the top of the femur. The iliacus lines the inside of the hip bone and attaches to the same point on the femur. Together, they pass directly through the pelvic cavity, lying adjacent to the pelvic floor muscles.
The connection isn’t incidental. It’s structural:
 The psoas and iliacus pass directly through the pelvic cavity, sharing fascial connections with the pelvic floor muscles.
The psoas and iliacus pass directly through the pelvic cavity, sharing fascial connections with the pelvic floor muscles.
Fascial Continuity
The psoas is enveloped in a fascial sheath that is continuous with the endopelvic fascia — the connective tissue that supports the pelvic organs and connects to the pelvic floor muscles. When the psoas fascia is restricted, it transmits tension directly to the pelvic floor. This isn’t a metaphor. It’s a physical, tissue-to-tissue connection.
Pelvic Tilt Influence
A persistently tight psoas pulls the lumbar spine forward. A tight iliacus pulls the pelvis itself into anterior tilt — the front of the pelvis drops, the back rises. This dual pull changes the orientation and resting tension of the pelvic floor muscles.
The pelvic floor can’t function optimally when the pelvis it’s attached to is being tilted from two directions at once. The iliacus is especially relevant here — it attaches directly to the pelvis, making its influence on pelvic positioning even more direct than the psoas.
The Diaphragm–Psoas–Pelvic Floor Axis
The diaphragm, psoas, and pelvic floor are connected through fascia and function as a pressure management system. When a breath is taken, the diaphragm descends, intra-abdominal pressure increases, and the pelvic floor must respond by yielding and returning.
If the psoas is rigid, this pressure system doesn’t work smoothly. The pelvic floor bears more load than it should, breath after breath, thousands of times per day.
Nerve Pathways
The nerves that travel to the pelvic floor — including pudendal nerve branches and the obturator nerve — pass through or near the psoas. When the psoas stays persistently tight, it can affect how these nearby structures feel, which is part of why pelvic tension can show up in places that seem unrelated to the muscle itself.
Why Pregnancy and Postpartum Make This Worse
The psoas and iliacus don’t get tight overnight. But pregnancy creates a perfect storm for persistent shortening of both muscles.
During Pregnancy
- The growing uterus pushes the psoas posteriorly, compressing it against the lumbar spine
- Hormonal changes (relaxin) increase ligamentous laxity, meaning the psoas and iliacus have to work harder to stabilize the pelvis
- Altered center of gravity increases lumbar lordosis, which shortens the psoas
- Reduced activity in later pregnancy means less dynamic lengthening of both muscles
After Delivery
- Frequent sitting for nursing and holding — hours per day in hip flexion
- Carrying on one hip creates asymmetric psoas and iliacus loading
- Sleep deprivation increases muscular tension systemically
- C-section recovery can create abdominal fascial restrictions that further limit psoas mobility
- Focus on pelvic floor recovery often doesn’t include psoas or iliacus assessment
The result: muscles that were already tight before pregnancy become significantly tighter after, and the pelvic floor recovery that follows addresses everything except the structures pulling on the system from above.
The Core Nexus was designed with separate tips for the psoas and iliacus — the two muscles most postpartum recovery programs overlook.
Signs the Psoas and Iliacus May Be Part of the Pattern
Not every case of persistent pelvic tension involves the psoas and iliacus. But the connection is worth looking into if any of the following are present:
- Pelvic floor therapy has helped but progress has plateaued
- Lower-back tightness accompanies the pelvic sensations
- Sensations worsen after prolonged sitting
- Anterior pelvic tilt persists despite corrective exercises
- Deep breathing feels restricted or incomplete
- One hip is noticeably tighter than the other
- Groin tightness or deep front-of-hip tension accompanies the pelvic sensations
- Kegels feel like they “don’t work” or the pelvic floor can’t fully relax after contracting
What to Do About It
Step 1: Talk to a Pelvic Floor PT About the Psoas
If a pelvic floor physical therapist is already involved in recovery, the psoas and iliacus should be part of the conversation. Many pelvic floor PTs already incorporate iliopsoas release into their practice, but it may not have been included in a specific plan. Asking about it explicitly can open a new direction.
Step 2: Add Psoas and Iliacus Release to the Daily Routine
This doesn’t replace pelvic floor work — it complements it by addressing the muscles that may be creating tension in the pelvic floor from above. Using a targeted release tool to apply sustained pressure to the psoas (through the abdomen) and iliacus (inside the hip bone), holding until the tissue softens and yields, followed by a gentle hip flexor stretch, can begin to change the pattern.
Step 3: Practice Diaphragmatic Breathing During Release
Because the psoas, diaphragm, and pelvic floor are fascially connected, conscious diaphragmatic breathing during psoas release can improve the release quality and help the pelvic floor respond simultaneously. This isn’t optional — it’s part of the mechanism. The breath creates a wave of pressure that helps the tissue let go.
Step 4: Be Patient with the Process
Postpartum psoas and iliacus tightness developed over months of pregnancy and recovery. It won’t ease overnight. Consistent daily practice often helps hip and back sensations and how the pelvic area feels over time.
How Recovery Approaches Compare
Most postpartum pelvic floor recovery focuses on the pelvic floor muscles directly. Here’s how common approaches compare when the psoas and iliacus are part of the pattern:
| Approach | Pelvic Floor | Psoas | Iliacus | Best For |
|---|---|---|---|---|
| Kegels | ✔︎ | ✘︎ | ✘︎ | Strengthening weak PF |
| Pelvic Floor PT | ✔︎ | ~ | ~ | Comprehensive pelvic floor work |
| Hip Flexor Stretching | ✘︎ | ~ | ~ | Surface-level flexibility |
| Foam Rolling | ✘︎ | ✘︎ | ✘︎ | Surface muscles only |
| Diaphragmatic Breathing | ✔︎ | ~ | ✘︎ | Pressure management |
| Targeted Psoas + Iliacus Release | ~ (indirect) | ✔︎ | ✔︎ | Releasing upstream tension |
| Combined: PF PT + Psoas/Iliacus Release + Breathing | ✔︎ | ✔︎ | ✔︎ | Full system approach |
Choosing the Right Release Tool
For psoas and iliacus release, the tool needs to reach both muscles — which have different locations and require different pressure approaches. The psoas responds to broader pressure through the abdomen, while the iliacus requires a narrower, angled approach to reach inside the hip bone.
The Core Nexus was designed with muscle-specific tips for exactly this — one shaped for the psoas, one contoured for the iliacus. Its self-rotating base allows angle adjustment without using hands, which is especially helpful during postpartum recovery when upper body strength may be limited or a baby needs to be held.
The Bottom Line
Pelvic floor recovery that plateaus often has a missing variable. The psoas and iliacus — two muscles that are fascially, structurally, and neurologically connected to the pelvic floor — are overlooked in most postpartum recovery programs. Pregnancy tightens them. Postpartum life keeps them tight. And their persistent tension pulls on the pelvic floor from above, keeping it in an overly tight, guarded state that doesn’t ease with strengthening alone.
Releasing both muscles — not just one — can change the equation. The psoas from the spine side. The iliacus from the pelvis side. Together, they address the upstream tension that standard pelvic floor work doesn’t reach.
Ready to release both muscles?
Endorsed by Clinicians
 Dr. Goñi
MD — Sports Medicine
Dr. Goñi
MD — Sports Medicine
 Dr. Sosa
DC — Chiropractic
Dr. Sosa
DC — Chiropractic
 Dr. Lang
PT, DPT — Physical Therapy
Dr. Lang
PT, DPT — Physical Therapy
 Dr. McHale
DC — Chiropractic
Dr. McHale
DC — Chiropractic
 Dr. Steph Dorworth
PT, DPT — Physical Therapy
Dr. Steph Dorworth
PT, DPT — Physical Therapy
Frequently Asked Questions
Yes. The psoas and iliacus are fascially connected to the pelvic floor through the endopelvic fascia. When these muscles are persistently tight, they transmit tension to the pelvic floor and alter pelvic alignment, both of which can keep the pelvic floor in an overly tight, guarded state that doesn’t fully relax.
Not necessarily one or the other. Kegels strengthen, but strengthening alone may not be the right starting point if the pelvic floor is already overly tight. If Kegels don’t seem to be helping or the pelvic floor can’t fully relax after contracting, working on the psoas and iliacus may help before strengthening becomes productive. A pelvic floor PT can assess what’s going on.
Gentle, progressive psoas and iliacus release is generally safe for postpartum women, but timing matters. Postpartum timing varies. Start gentle psoas and iliacus work only after initial recovery and clinician clearance, especially after C-section or delivery complications.
Many people tell us they notice initial changes once release becomes part of a consistent daily routine. A more meaningful difference in how the area feels tends to build gradually, since psoas and iliacus tightness developed over months of pregnancy and the postpartum period. Consistency matters more than intensity — brief daily sessions tend to outperform occasional deep sessions.
The psoas and iliacus attach to different structures (spine vs. pelvis) and require different pressure approaches. The psoas needs broader pressure through the abdomen; the iliacus needs a narrower, angled approach to reach inside the hip bone. A single generic tip can’t effectively reach both. Tools with muscle-specific tips — like the Core Nexus — are designed to address each muscle with the correct pressure profile.
Absolutely. While this article focuses on the postpartum period, the psoas-pelvic floor connection exists regardless of sex. Men who carry persistent pelvic and deep-hip tension can also benefit from addressing psoas and iliacus tightness as part of a broader mobility routine.
Nexus Health Tools designs precision instruments for targeted myofascial release, built on real anatomy and endorsed by clinicians. Every product is engineered in the USA to address the muscles most tools miss.
This article is for educational purposes and does not replace evaluation by a pelvic floor physical therapist. If you have significant pelvic floor symptoms, work with a qualified provider.