How Physical Therapists Use Self-Myofascial Release for Persistent Tightness (And How You Can Too)

Core Nexus
Two muscles. Two tips. One tool — releases both the psoas and the iliacus.
📖 In This Article
 Dr. Steph Dorworth (PT, DPT) with the Core Nexus — one of five clinicians who endorse the tool for professional and home myofascial release.
Dr. Steph Dorworth (PT, DPT) with the Core Nexus — one of five clinicians who endorse the tool for professional and home myofascial release.
If you've ever had a physical therapy session where the therapist pressed into a tight spot, held it for what felt like forever, and then suddenly the tension you'd been carrying for months just… released — you've experienced myofascial release.
And if you've ever wondered why you can't replicate that feeling at home with a foam roller and some YouTube stretches, you're not alone. There's a reason it works when a PT does it and doesn't when you try it yourself — and it's not because PTs have magic hands.
It's technique. Specifically, it's understanding what fascia is, why it matters, and how sustained targeted pressure does something that stretching physiologically cannot.
What Fascia Actually Is (Not What Instagram Thinks)
Fascia has become a wellness buzzword. Social media is full of people “scraping” their IT bands, “breaking up” scar tissue with metal tools, and claiming to “release” fascia by rolling on foam cylinders.
Most of that is incomplete at best.
Fascia is a continuous web of connective tissue that surrounds and interconnects every muscle, organ, nerve, and bone in the body. Think of it as the biological shrink-wrap that holds everything in place and allows structures to glide past each other during movement.
When fascia is healthy, it's hydrated, flexible, and allows smooth movement between tissue layers. When it's unhealthy — from prolonged tension, immobility, or strain — it becomes dehydrated, sticky, and restricted. Layers that should glide freely get “glued” together. This is what practitioners mean by fascial restriction or fascial adhesion.
Here's what matters for this topic:
Fascia has its own nerve supply. It contains mechanoreceptors (sensors that detect pressure and stretch) and nociceptors (sensors). This means fascia can generate sensation independently — it's not just a passive wrapper. Research published in the Journal of Bodywork and Movement Therapies has shown that fascial tissue has a higher density of these receptors than muscle tissue in many areas of the body.
Fascia responds to sustained pressure differently than muscle. Muscles respond to stretch — lengthen them, and they temporarily increase in length. Fascia responds to sustained compression — apply pressure for an extended hold, and it undergoes a process called thixotropy: the tissue transitions from a gel-like state (stiff, restricted) to a more sol-like state (fluid, mobile). This is a physical property of the collagen matrix, not a muscle response.
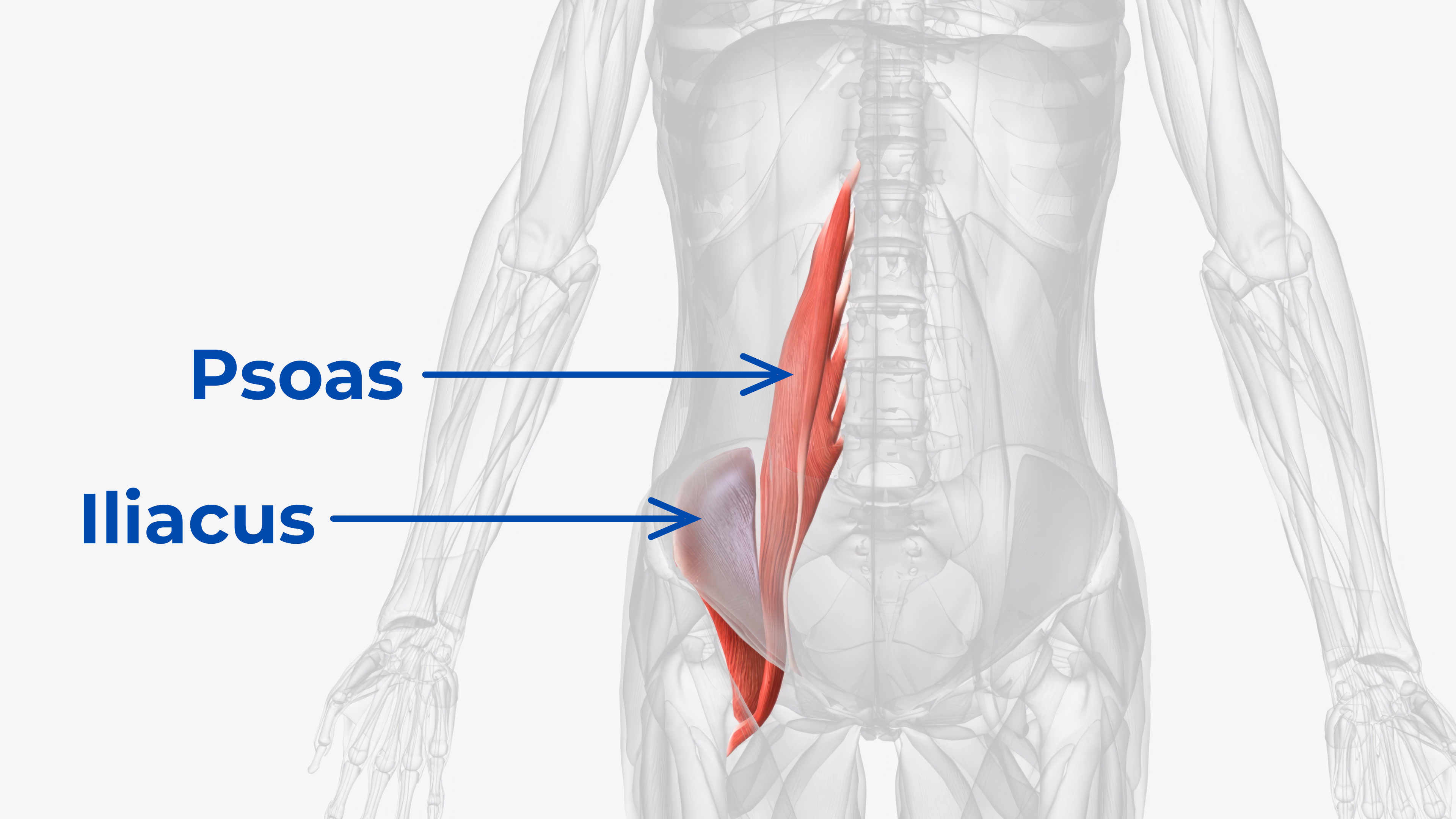 The psoas and iliacus: two distinct muscles requiring two distinct approaches for effective myofascial release.
The psoas and iliacus: two distinct muscles requiring two distinct approaches for effective myofascial release.
How Physical Therapists Actually Do It
Here's the approach, demystified — the same method used by the PTs who endorse the Core Nexus and use it themselves:
Step 1: Assessment
The PT palpates (manually examines) the tissue, looking for areas of restriction. They're feeling for:
- Tight spots — sensitive spots within a taut band of muscle/fascia that can refer sensation to other areas
- Fascial adhesions — areas where tissue layers are stuck together and don't glide normally
- Tissue texture changes — areas that feel “ropy,” “gritty,” or excessively dense compared to surrounding tissue
A skilled PT can feel the difference between healthy tissue and restricted tissue within seconds. This is one of the key skills that takes years to develop — and it's why PTs get results that foam rollers can't replicate.
Step 2: Sustained Pressure
Once a restriction is identified, the PT applies pressure — usually with their thumb, elbow, or a specialized tool — directly into the restricted area. The pressure is moderate to firm. Not brutal. Not “more force is better.” The goal is to engage the tissue without triggering a protective guarding response.
The key variable is time, not force.
The hold continues long enough for both thixotropic change (fascia softening from gel to sol) and neurological relaxation (the nervous system recognizing sustained input as safe and allowing the contraction to release). This process takes seconds to minutes depending on the depth and how long the restriction has been present.
Step 3: Movement Integration
After releasing a restriction, the PT has the client move. Walk, squat, rotate — something that uses the muscle in its new, released state. This “teaches” the nervous system the new range of motion and reduces the likelihood of the tissue snapping back to its restricted pattern.
This step is what most people skip at home. Release without movement integration is temporary. Release followed by functional movement is durable.
The Core Nexus — dual muscle-specific tips engineered for the same targeted sustained pressure physical therapists apply.
Why Most At-Home Attempts Fall Short
When people try myofascial release at home, three things typically go wrong:
1. Wrong Tool for the Target
Foam rollers are effective for superficial muscles (quads, IT band, upper back) but cannot reach deep structures like the psoas, iliacus, or suboccipitals. These muscles lie beneath multiple tissue layers — the psoas is the deepest hip flexor in the body, running from the lumbar spine through the abdomen. No foam roller can apply specific, targeted pressure at that depth. Using the wrong tool for the wrong muscle is effort without effect.
2. Not Enough Sustained Pressure
Rolling back and forth doesn't produce thixotropic change. It stimulates mechanoreceptors and temporarily reduces the sensation — which is why it feels good in the moment — but it doesn't change the fascial restriction. Effective release requires sustained, static pressure held long enough for the tissue to actually respond. Most people move too quickly, mistake temporary easing for better carryover, and wonder why the tightness returns within hours.
3. Lack of Precision
Physical therapists can feel exactly where the restriction is and maintain pressure on that specific point for as long as the tissue needs. At home, without palpation training, people tend to press in the general vicinity rather than on the specific restriction. A tool with anatomically shaped contact points partially solves this problem by guiding pressure to the anatomically correct location — but the tool must be designed for the specific muscle being targeted.
 Muscle-specific tips: the broader psoas tip applies pressure through the abdomen; the narrower iliacus tip angles precisely inside the hip bone.
Muscle-specific tips: the broader psoas tip applies pressure through the abdomen; the narrower iliacus tip angles precisely inside the hip bone.
How to Do It Right at Home
For the Psoas and Iliacus
The two deepest, most commonly restricted hip flexors require targeted pressure that foam rollers and general tools cannot provide. The psoas needs broader pressure applied through the abdomen. The iliacus needs a narrower, angled approach inside the hip bone. These are different muscles in different locations — they need different contact surfaces, and both are worth working on in the same session for a fuller release pattern.
Releasing one while the other stays tight is the most common reason self-release work produces only temporary easing. The tension simply transfers between the two muscles. This is why the Core Nexus was designed with two distinct tips: one shaped for the psoas, one for the iliacus, with a stable base and self-rotation that maintains optimal pressure as the body naturally shifts during the hold.
For the Suboccipitals
The four small muscles at the base of the skull respond to gravity-assisted pressure from a cradle-style tool. Lie on the back, position the tool at the skull base, and allow the weight of the head to provide the sustained compression. The Black Swan was designed for this — dual cradles that conform to the occipital ridge and hold position as the suboccipital muscles release.
The Home Protocol
- Identify the primary restriction — Where is the tension? Hips and lower back → psoas and iliacus. Neck tightness and base-of-skull tension → suboccipitals.
- Apply sustained pressure — Hold until the tissue responds. Don't roll. Don't bounce. Just hold and breathe. The release typically occurs within 1–3 minutes of sustained contact.
- Move after releasing — Walk, do a few bodyweight squats, perform a hip hinge. Integrate the new range of motion immediately so the nervous system retains it.
- Be consistent — Regular daily practice produces better results than occasional long sessions. Long-standing fascial restriction develops over months or years; it tends to ease with consistent, targeted input.
Ready to bring targeted myofascial release into your daily routine at home?
The Bottom Line
The difference between what physical therapists do and what most people attempt at home isn't knowledge — it's tool specificity and time. PTs use the right tool for the right muscle and hold long enough for the tissue to actually change. That's the formula.
The goal isn't perfection. The goal is consistency. Regular practice targeting the right muscles at the right depth with appropriate sustained pressure, followed by movement integration. That's the protocol PTs use — and it's fully replicable at home with the right equipment.
Five clinicians across MD, DC, PT, and DPT credentials have endorsed the Core Nexus for exactly this: bringing professional-quality myofascial release out of the PT office and into daily home practice.
Endorsed by Clinicians
 Dr. Goñi
MD — Sports Medicine
Dr. Goñi
MD — Sports Medicine
 Dr. Sosa
DC — Chiropractic
Dr. Sosa
DC — Chiropractic
 Dr. Lang
PT, DPT — Physical Therapy
Dr. Lang
PT, DPT — Physical Therapy
 Dr. McHale
DC — Chiropractic
Dr. McHale
DC — Chiropractic
 Dr. Steph Dorworth
PT, DPT — Physical Therapy
Dr. Steph Dorworth
PT, DPT — Physical Therapy
Frequently Asked Questions
Self-myofascial release (SMR) uses sustained targeted pressure to address fascial restrictions — areas where connective tissue has become dehydrated, stiff, or adhered. Stretching primarily addresses muscle length by lengthening muscle fibers. SMR targets the fascia surrounding muscles and undergoes a different physiological process called thixotropy, where sustained compression shifts the fascial matrix from a stiffer gel-like state to a more fluid state. You need both, but they accomplish different things.
Physical therapists use palpation to identify the exact location of a restriction and apply sustained, static pressure directly to that point. Foam rollers produce rolling compression across a broad surface area and don't achieve the sustained contact necessary for thixotropic change in fascia. PTs also guide movement integration immediately after release — a critical step most people skip at home.
Most restrictions respond within 1–3 minutes of sustained static pressure. The key signal is a perceptible softening or “release” in the tissue — the sensation of the restriction yielding under pressure. Holding too briefly (under 30 seconds) primarily stimulates mechanoreceptors without producing lasting fascial change. Holding past the release point provides diminishing returns. Moderate pressure held for 90–120 seconds is a reliable starting point for most restrictions.
No. The psoas originates at the lumbar vertebrae and runs through the abdominal cavity — it is the deepest hip flexor in the body. The iliacus lines the inside of the hip bone. Both muscles require specific approaches to reach: broader compression through the lower abdomen for the psoas, and a narrower angled approach inside the ASIS (anterior superior iliac spine) for the iliacus. Foam rollers apply superficial compression to whatever tissue is closest to the skin. Neither muscle is accessible through a foam roller.
Movement integration is the step performed immediately after releasing a restriction to reinforce the new range of motion with functional movement. After sustained pressure releases a fascial restriction, the nervous system has temporarily learned that the new position is safe. Active movement in that new range — walking, squatting, hip hinges, or rotation — consolidates the neurological adaptation and reduces the likelihood of the tissue reverting to its restricted pattern. Skipping this step turns temporary easing into better carryover.
Daily practice tends to work better than occasional sessions for long-standing fascial restriction. Persistent tightness typically develops over months or years of postural patterns, immobility, or repeated stress — and tends to ease with consistent, targeted input rather than infrequent intensive sessions. A 10–15 minute daily protocol targeting the primary restriction areas tends to work better than a 45-minute session once a week. Consistency is the highest-leverage variable in self-myofascial release.
Nexus Health Tools designs precision instruments for targeted myofascial release, built on real anatomy and endorsed by clinicians. Every product is engineered in the USA to address the muscles most tools miss.